
Once your doctor confirms an NHL diagnosis, he or she will determine the extent of your disease's progression by staging. Staging helps your doctor predict the disease's progression and develop a treatment plan.
Staging Tests
Imaging Tests
Your doctor conducts one or more imaging tests along with a physical exam, to evaluate:
- The location and distribution of lymph node enlargement
- Whether organs other than the lymph nodes are involved
- If there are very large masses of tumors in one or more site(s)
Imaging tests include:
- Chest x-rays
- CT (computed tomography) scan
- Magnetic resonance imaging (MRI)
- Positron emission tomography-computed tomography (PET-CT) scans
Click here to read about each test.
Blood Tests
Blood tests are used to determine whether lymphoma cells are present in the blood; check for indicators of disease severity by examining blood protein levels; assess kidney and liver functions; and measure important biological markers, which are helpful prognostic indicators for several NHL subtypes. Blood tests include:
- Complete blood count (CBC) - This test measures different components of the blood, including counts of red blood cells, white blood cells and platelets.
- Comprehensive metabolic panel - This test often includes tests for up to 14 chemicals. Chemicals in the blood come from the liver, bone and other organs. Abnormal levels can be caused by cancer or other health problems.
- Beta2 microglobulin - Beta2 microglobulin is a small protein made by many types of cells, including lymphoma cells. High levels of this protein may be an indication that treatment is needed right away.
- Lactate dehydrogenase (LDH) - LDH is a protein that is found in most cells. When a cell is damaged, LDH is released into the bloodstream. Thus, when associated with a cancer, a high LDH level may be a sign that treatment is needed soon.
- Hepatitis testing - The presence of hepatitis B or hepatitis C can be important considerations when treating certain types of lymphoma. Hepatitis B can become active again due to cancer or some of its treatments. Hepatitis C may diminish the effectiveness of therapy.
- HIV (human immunodeficiency virus) testing - If HIV is present, treating it can be an important part of how NHL is managed.
- Uric acid testing - This test measures the amount of uric acid in the body. When cancer cells breakdown and die, they release substances into the blood. If the cancer cells breakdown too quickly, the kidney’s cannot remove these substances from the blood. An increased level of uric acid can lead to tumor lysis syndrome (TLS).
- Antibody testing - Depending on the type of NHL, people may have either low levels of antibodies or very high amounts of tumor-specific antibodies.
Click here to read more.
Bone Marrow Biopsy
Most patients diagnosed with NHL undergo a bone marrow biopsy to make sure there is no spread of the disease to the bone marrow and to evaluate the use of specific therapies including radioimmunotherapy (a combination of radiation therapy and immunotherapy). A bone marrow biopsy may not always be required for patients with early-stage disease who also have low-risk features.
Click here to read more.
Heart Tests
Some cancer treatments can damage the heart. So, members of the treatment team may want to determine how well a patient’s heart functions before he or she starts a specific treatment. Tests include:
- An echocardiogram—An imaging test that uses ultrasound technology to create a picture of the heart
- A multigated acquisition (MUGA) scan—This scan measures how well the heart pumps blood. A radiotracer substance is injected into a vein. Pictures of the heart are taken with a special camera that detects the radiation released by the tracer.
Other Tests
Some tests are associated with a specific subtype and are not necessary for all patients with NHL. Examples of specific testing include:
- Full evaluation of the gastrointestinal (GI) tract, including upper and lower endoscopies for patients who have disease involving the GI tract, such as mantle cell lymphoma (MCL) and gastric mucosa-associated lymphoid tissue (MALT) lymphoma
- Colonoscopy for patients with MCL (routine colonoscopy is important for all persons beginning at age 50, or earlier if there is a family history of colon cancer or other risk factors)
- Testicular ultrasound for patients who have a testicular mass
- Spinal tap (lumbar puncture) and/or MRI of the brain or spinal column may be required for patients with certain subtypes or symptoms that suggest central nervous system (CNS) involvement
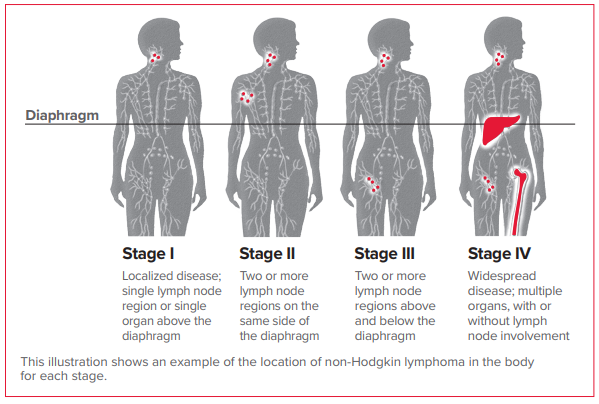
Staging
Keep in mind that the designation “stage IV” does not have the same implications in NHL as it does for many other types of cancer. Non-Hodgkin lymphoma does not necessarily start at stage I and then progress to stage II, and so forth. In lymphoma, the stage identifies the specific location of the disease. It also does not reflect how well or poorly the patient will respond to treatment. A disease diagnosed as stage IV NHL may be highly treatable, depending on the specific subtype.
Lugano Modification of Ann Arbor Staging Systems (for primary nodal lymphomas)
| Stage | Involvement | Extranodal (E) status |
|---|---|---|
| Limited | ||
| Stage I | One node or a group of adjacent nodes | Single extranodal lesions without nodal involvement |
| Stage II | Two or more nodal groups on the same side of the diaphragm | Stage I or II by nodal extent with limited contiguous extranodal involvement |
| Stage II bulky | II as above with "bulky" disease | Not applicable |
| Advanced | ||
| Stage III |
Nodes on both sides of the diaphragm Nodes above the diaphragm with spleen involvement |
Not applicable |
| Stage IV | Additional non-contiguous extralymphatic involvement | Not applicable |
When all the diagnostic and staging tests are completed, the doctor will evaluate the information, identify the NHL subtype, determine which areas of the body are involved and begin to discuss treatment options with the patient.
Related Links
- Lab and Imaging Tests
- Download or order The Leukemia & Lymphoma Society’s free booklets: